

The interscalene blocks works like a charm for most of these abscesses. However, the interscalene block has significant potential complications including paralysis of the diaphragm. While a technically very easy block, you need to know what you are doing and be prepared to avoid nerve injury, toxicity and other potential harms from the procedure.
Selective block of the axillary nerve avoids many of the risks associated with brachial plexus blocks and provides just about complete anesthesia for the deltoid region.
The axillary nerve forms from the ventral rami of C5 and C6 and innervates the deltoid, the teres minor and the long head of the triceps brachii as well as providing sensory innervation to the shoulder joint and the skin covering the the deltoid region or "regimental patch" area on the arm. The Axillary nerve travels through the quadrangular space adjacent to the posterior circumflex humeral artery where it can be well visualized for blockade. A perfect indication for axillary nerve block is the injection drug use caused deltoid abscess commonly seen in emergency departments.
Big abscesses may extend into the border innervations. The most superior aspect of the shoulder or "cape" will be innervated by the supraclavicular nerves. Down the arm, the inferiorly axillary innervation borders with the radial nerve territory. Medially towards the axilla there is innervation from the medial antebrachial cutaneous nerve (C8/T1) and the intercostobrachial nerve (T2).





The easiest way to perform this block is to have the patient laying down prone. If the patient is seated, the it can be a struggle to keep the probe from sliding out from you. Prone positioning, using an extension tubing makes the procedure quite comfortable.
Approach from cephalad to caudad in the the roughly sagittal plane. The nerve itself is normally about 4cm inferior to the acromion and 2-4cm deep.

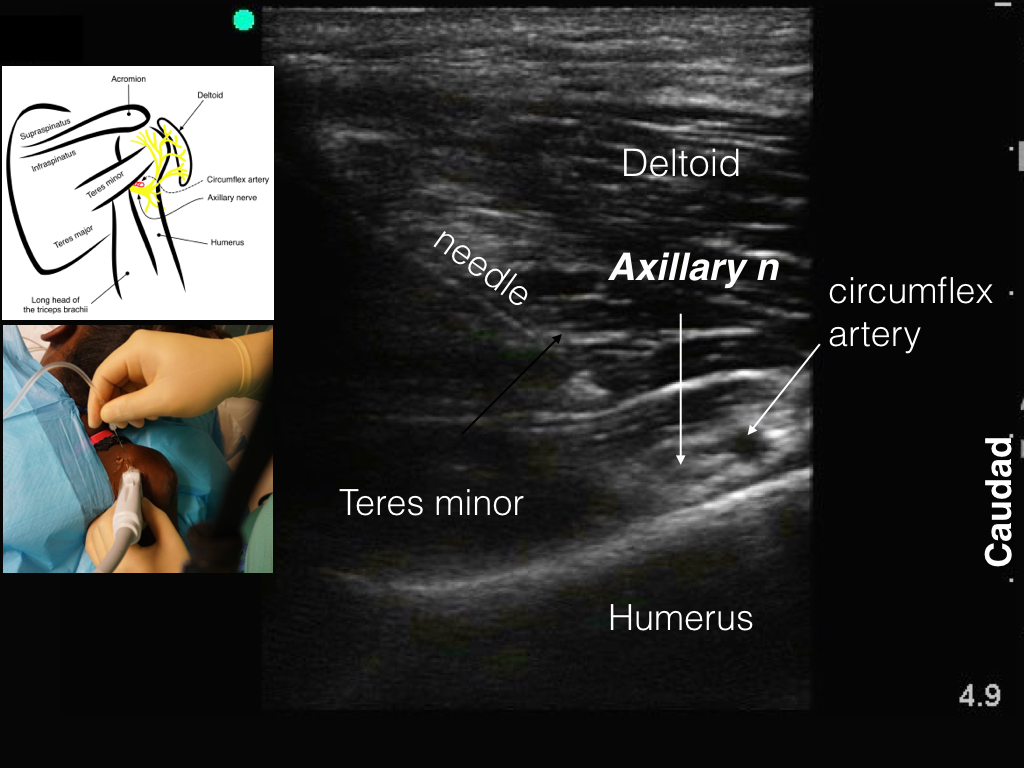
The axillary nerve is consistently found in the quadrangular space as it loops around to innervate the deltoid muscle. With the ultrasound transducer roughly in-line with the long axis of the humerus, look for the characteristic pattern of the teres minor muscle tucking in like a little thumb from the medial side, underneath the large deltoid muscle. At the tip of the "thumb" the axillary nerve runs adjacent to the circumflex artery. It has a typical "honeycomb" appearance.
Local anesthetic filling the quadrangular space

Axillary nerve, surrounded by local anesthetic.

Successful and painless incision and drainage without sedation (patient slept through procedure, no meds given)

REFERENCES
- Checcucci, G., Allegra, A., Bigazzi, P., Gianesello, L., Ceruso, M. & Gritti, G., 2008, A new technique for regional anesthesia for arthroscopic shoulder surgery based on a suprascapular nerve block and an axillary nerve block: an evaluation of the first results, Arthroscopy: The Journal of Arthroscopic & Related Surgery, 24(6), pp. 689-96.
- Kim, Y.A., Yoon, K.B., Kwon, T.D., Kim, D.H. & Yoon, D.M., 2014, Evaluation of anatomic landmarks for axillary nerve block in the quadrilateral space, Acta anaesthesiologica Scandinavica, 58(5), pp. 567-71.
- Nam, Y.S., Jeong, J.J., Han, S.H., Park, S.E., Lee, S.M., Kwon, M.J., Ji, J.H. & Kim, K.S., 2011a, An anatomic and clinical study of the suprascapular and axillary nerve blocks for shoulder arthroscopy, Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons ... [et al.], 20(7), pp. 1061-8.
- Nam, Y.-S., Jeong, J.-J., Han, S.-H., Park, S.-E., Lee, S.-M., Kwon, M.-J., Ji, J.-H. & Kim, K.-S., 2011b, An anatomic and clinical study of the suprascapular and axillary nerve blocks for shoulder arthroscopy, Journal of Shoulder and Elbow Surgery, 20(7), pp. 1061-8.
- Rothe, C., Asghar, S., Andersen, H.L., Christensen, J.K. & Lange, K.H., 2011, Ultrasound-guided block of the axillary nerve: a volunteer study of a new method, Acta anaesthesiologica Scandinavica, 55(5), pp. 565-70.